






















.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Counterpoint
Hal Andrews | December 4, 2024With the passage of time, artists occasionally seem to have predicted the future, like Ray Bradbury or Aldous Huxley or H.G. Wells. In the aftermath of the 2024 Presidential Election, I have heard several Beltway denizens referencing The Matrix and lamenting how many people were “red-pilled,” seemingly unaware of what their use of that term implies about them.
As for me, the 2024 Presidential Election recalls Peter Finch’s memorable meltdown as news anchor Howard Beale in the 1976 film Network. I think every health economy stakeholder would do well to watch the clip and imagine that you are the target of the indignation, because there is a good chance that you are about to be.
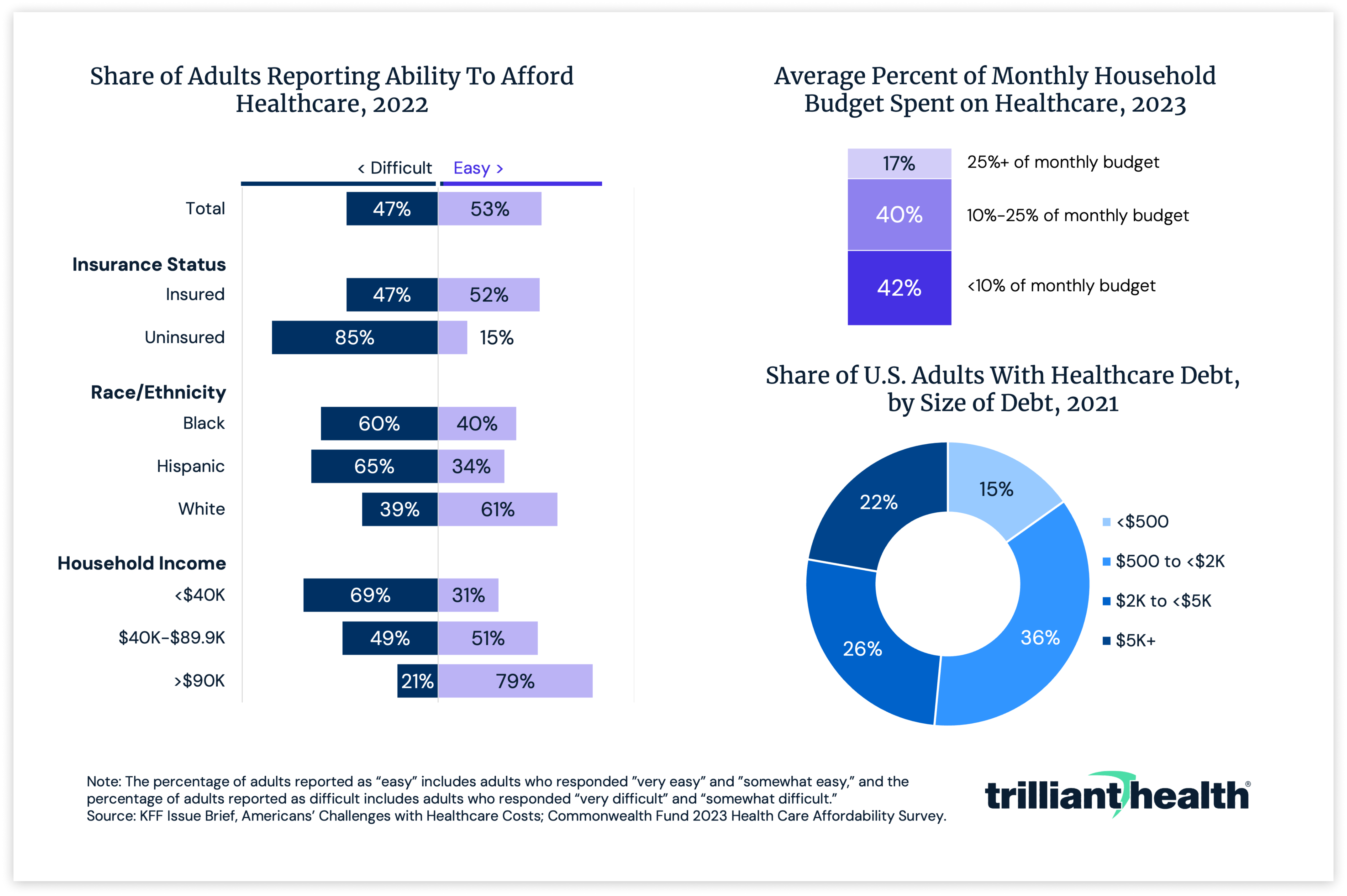
Why? Because Americans cannot afford the American healthcare system.
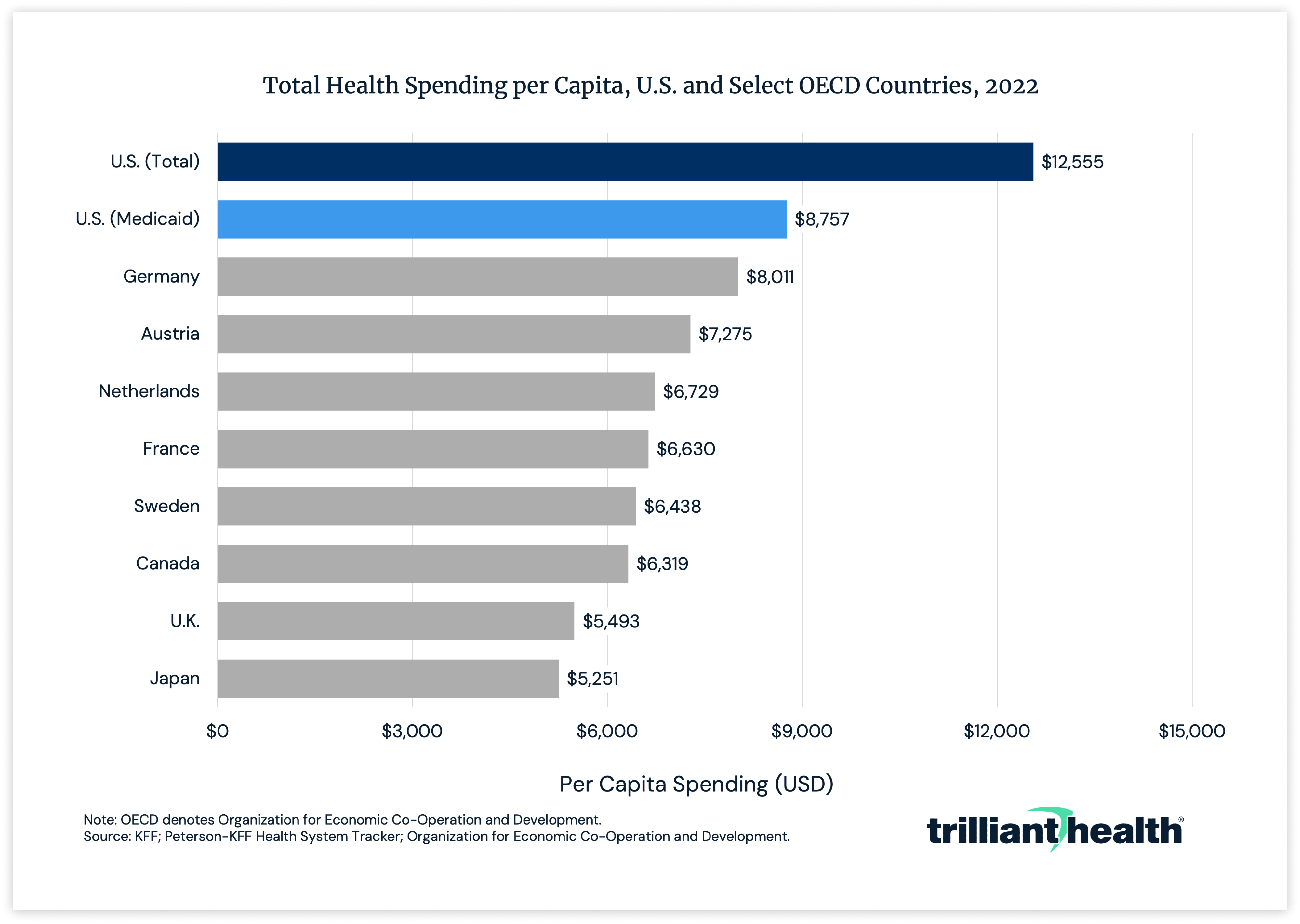
The reason is that the U.S. health economy represents 45% of the global health economy.1,2 In fact, America’s per capita Medicaid spending is higher than any other country’s total per capita health spending.
Despite all that money, most Americans are not quite as enamored with physicians and hospitals as much as old, rich, educated white men, and even The New York Times agrees.3
.png)
Employer-Sponsored Health Insurance: The Parasitic Host of the Health Economy
Perhaps some of that lack of trust owes to the fact that America’s health system is inequitable. Much has been written about race being the cause of that inequity, although Richard “Buz” Cooper, M.D., argued convincingly that poverty was the root cause. Jesus said, “The poor you will always have with you,” and America is no exception, and poverty knows no geographic bounds. Unsurprisingly, therefore, a statute based on income – the Affordable Care Act (ACA) – is the only policy that has meaningfully impacted health equity in the past 25 years.
Ironically, nothing demonstrates the inequity of the U.S. health system like the ACA, which implicitly establishes the baseline of what the Federal government believes is necessary for an individual to purchase health insurance coverage. As a result, everything else is, as my Gen Z children like to say, “extra.”
For both FY 2024 and FY 2025 HHS requested “$2.3 billion to operate the Federally Facilitated Marketplace” (the “Marketplace”), and 21.3M people enrolled in the Marketplace in FY 2024, implying a $108 per capita cost for the Federal government to enroll an individual in health insurance.4,5 Notably, the fact that CMS neither prohibits nor regulates commissions payments on the Marketplace demonstrates that neither Congress nor CMS believes that a broker is essential to an individual obtaining coverage.
The health policy experts who have decried for decades that 30% of healthcare spending is waste have been strangely silent about addressing the root cause of the waste that does exist: America’s employer-sponsored health insurance system. Likewise, the health policy experts decrying the inequity in the U.S. health economy have rarely, if ever, articulated employer-sponsored health insurance’s role in perpetuating that inequity.
The problem isn’t that employer-sponsored health insurance is unfair, but rather that employer-sponsored health insurance is the lifeblood of the waste in the health economy. Ironically, the ACA’s medical loss ratio mandates catalyzed that waste by removing incentives for health insurers to limit costs.
As the CEO of a self-insured employer that analyzes healthcare data, I despise every aspect of my company’s role in underwriting health insurance for our employees. I know that I can only dream of our company spending only $108 per employee to complete open enrollment, even as I wonder why it should cost that much. I am both annoyed and astonished at the power that employers and health insurers have granted to health benefits brokers and consultants, who are the healthcare version of Woody from Toy Story, repeating phrases like “expect an increase of 15-20%” and “narrow networks” and “direct contracting” when you pull their string. I can only conclude that the 200%-800% variance in negotiated rates paid in the same market for the same service by the same health insurer reveals either incompetence or indifference about addressing the cost of their provider networks.
As the CEO of a self-insured employer, I am mad as hell about this waste and grift that exists solely because of – and at the expense of – employers who provide health insurance benefits. While I am perplexed as to why Fortune 500 chief financial officers haven’t had a Howard Beale moment about being the parasitic host of the entire U.S. health economy, I understand what might happen if they do.
First Principles and Black Swan Events
Peter Drucker noted that “most innovations in public service institutions are imposed on them either by outsiders or by catastrophe.”6 To the Beltway establishment, President-elect Trump’s “kitchen cabinet” and announced nominees are the very definition of outsiders. Those outsiders – like Elon Musk and Robert F. Kennedy Jr. and Marty Makary, M.D., and Jay Bhattacharya, M.D. – believe that the U.S. healthcare system is badly broken, which makes them the natural enemy of many health economy stakeholders.
In The Art of War, Sun Tzu said this:
“The art of war teaches us to rely not on the likelihood of the enemy’s not coming, but on our own readiness to receive him; not on the chance of his not attacking, but rather on the fact that we have made our position unassailable.”7
There is no health economy stakeholder whose position is unassailable because healthcare inflation is unrelenting.
.png)
The Matrix is analogous to healthcare in that Americans are trapped in a healthcare system that has an insatiable thirst for their financial resources in the form of Medicare taxes and income taxes and health insurance premiums and deductibles and co-pays and co-insurance. Health economy stakeholders have “blue-pilled” the American public into believing that we are delivering a product that is safe and high quality, if expensive.
Importantly, despite the apparent lack of a coherent health policy approach, the first Trump Administration implemented price transparency, which will ultimately become the most transformational healthcare policy since the introduction of DRGs in 1983. Whether a coherent health policy approach emerges in the incoming Trump Administration, the leaders of the “Department of Government Efficiency” have a mantra – “first principles” – and a “soft target” in departments that represent 24% of Federal expenditures.8
“First-principles” thinking is one of the best ways to reverse-engineer complicated problems. Sometimes called “reasoning from first principles,” the idea is to break down complicated problems into basic elements and then reassemble them from the ground up. A first principle is a foundational proposition or assumption that stands alone. For example, when Elon Musk wanted to make space travel more affordable, he broke down the cost of rockets to their material constituents and realized that they were only a small fraction of the total expense. He decided to create SpaceX and build rockets from scratch, deviating from the traditional, expensive manufacturing methods.
In November 2023, I wrote about how Elon Musk might transform healthcare with first principles. In summary, the less that your business has adopted first principles, the more exposed your business is to disruption.
Similarly, the more instinctively dismissive you are of the incoming administration, the more that you should contemplate “black swan events” that could impair your business. A black swan event is a “high-impact event that is difficult to predict under normal circumstances but that in retrospect appears to have been inevitable.”9
Captain Phillips is based on a black swan event of the hijacking of the cargo ship Maersk Alabama. Nobody thought it possible that four pirates on a speedboat could hijack a cargo ship that was 500 feet long and 90 feet tall, but everyone who saw the movie remembers the scene in which the Somali pirate looks at Captain Phillips, played by Tom Hanks, and says, “Look at me. Look at me. I’m the captain now.” If your core business extracts most of its profits from employer-sponsored healthcare but does not involve treating patients, then your business is analogous to the Maersk Alabama, and you are like Captain Phillips.
What health economy stakeholders fail to understand – ultimately at their peril - is that their most important customer – employers – face relentless challenges in their industry sector to deliver more value to their customers. That increased value takes many forms: more “stuff” for the same price, the same “stuff” for a lower price and – gasp – more “stuff” for a lower price. The fact that health economy stakeholders want to provide the same, stunningly average, “stuff” for an ever-increasing price doesn’t make sense. The decades-long reliance by health economy stakeholders on price increases has induced an anesthetic-like stupor numbing them to the importance of delivering value in healthcare’s negative-sum game, which, in turn, increases the fragility of their business models, a hallmark of the “victims” of black swan events.
I don’t know what, if any, new initiatives the incoming Trump Administration will pursue related to the health economy. I also don’t know whether employers will demand that health economy stakeholders deliver more value for money as they could and, under ERISA and Delaware law, arguably should.
On the other hand, it is possible that no President has been more concerned about his legacy than Donald J. Trump. Just as the Affordable Care Act defines President Obama’s legacy, a radical change to the employer-sponsored healthcare system would define President Trump’s legacy.
In August, I wrote of the creative destruction that would be unleashed in the health economy if $1.0T was converted from premiums and deductibles and co-pays and co-insurance into salaries and wages if Congress eliminated the tax deduction for employer-sponsored health insurance, perhaps the ultimate black swan event.
Congress has implemented three major enactments of the Internal Revenue Code (the “Code”), in 1939, 1954 and 1986. The Tax Reform Act of 1986 was transformative in many ways, but cataclysmic for those participating in tax shelters for real property and oil and gas.
History suggests that the Code is due for a comprehensive overhaul, and anyone who knows anything about first principles will know that there are opportunities to simplify a framework that originates in a statute that exceeds 2,000 pages. Whether the ACA effectively undermines whatever tax policy basis exists for the employer-sponsored health insurance tax deduction is an interesting question. While employers are accustomed to being the focal point of the U.S. health economy, whether they want to be is a different question.
These questions, and others, present a potential black swan event for health economy stakeholders. What if, in 2025, Congress undertakes a “first principles” overhaul of the Internal Revenue Code of 1986, and what if employers decided to “trade” the tax deduction for employer-sponsored healthcare for lower corporate tax rates? What if the Department of Government Efficiency convinces President Trump that the first principle of a consumer-driven health economy is to allow individuals to use their own money to make individual decisions about their physician or hospital with the benefit of price transparency? What if Congress, with the hearty support of every state, county and municipality, changes the provisions to Section 501(c)(3) of the Code relied on by health systems that are tax-exempt, or as Senator Rick Scott used to say, "non-tax paying"?
I don’t think any of these things have a high probability of occurring, but I have considered them. Have you?