In 1840, William Farr submitted a letter to the Registrar-General regarding his observations on the causes of death in England and Wales in the year 1838. In his 28-page abstract, Mr. Farr had occasion to observe certain characteristics of the virulent smallpox outbreak in England during that year. Mr. Farr observed that the
“diseases of the epidemic class follow laws of their own; they remain nearly stationary during months, years, and, as we learn from medical history, centuries; then suddenly rise, like a mist from the earth, and shed desolation on nations – to disappear as rapidly or insensibly as they came.” [1]
At a moment in time when the media seeks guidance from NBA owners about non-pharmaceutical interventions to combat global pandemics and a former CMS administrator uses vulgar language to suggest that empathy is the foundational element of progress against a virus, it seems rather quaint to consider the laws of epidemiology. Call us old-fashioned, but we think that Farr’s Law of Epidemics might have something to offer in the current environment.
To be clear, we are not the first to suggest the wisdom of considering Farr’s Law in the context of Covid-19. In April of this year, Carl Heneghan and Tom Jefferson of The Centre for Evidence-Based Medicine wrote that “[u]nderstanding William Farr’s contribution to outbreaks is crucial to understanding our way out of this pandemic.” [2] We agree.
In his report, Mr. Farr noted the following:
The pestilences of ancient history, the plagues of England, cholera, influenza, smallpox, and typhus, are examples of this peculiar tribe of diseases. Epidemics have furnished much matter for discussion, and still offer large scope for inquiry. They have been attributed to terrestrial emanations, to the influence of the stars, to mysterious change in the atmosphere, to heat, to animalcules, to deteriorated food, to contagion; and acting upon the latter doctrine, it has been assumed that the prohibition of direct intercourse with districts in which they prevailed would protect the inhabitants of a country from invasion.
The problem for solution is, Why do the five deaths become 10, 15, 20, 31, 58, 88 weekly, and then progressively fall through the same measured steps? This difficulty has presented itself in the history of plague and of contagious diseases of every description; but it has generally been disposed of summarily, by the hypothesis that the disease is always introduced from without, and spreads naturally, like a conflagration. When the plague broke out, that is, became epidemic, in Cairo, the Egyptians asserted that it came from Ethiopia; when it decimated Constantinople, it was ascribed to merchandise or vessels from Egypt.
Epidemics appear to be generated at intervals in unhealthy places, spread, go through a regular course, and decline; but of the cause of their evolutions no more is known than of the periodical paroxysms of ague. The body, in its diseases as well as its functions, observes a principle of periodicity; its elements pass through prescribed cycles of changes, and the diseases of nations are subject to similar variations.” [3]
What Mr. Farr observed is this:
If the latent cause of epidemics cannot be discovered, the mode in which it operates may be investigated. The laws of its action may be determined by observation, as well as the circumstances in which epidemics arise, or by which they may be controlled. Amidst the apparent irregularities of the epidemic of smallpox, and its eruptions all over the kingdom, it was governed in its progress by certain general laws. [4]
In summary, what is now known as Farr’s Law is that epidemics rise and fall at a predictable rate that can be calculated by a single mathematical formula approximated by a bell-shaped curve. [5][6]
Farr’s description of smallpox in England in 1838 is certainly analogous to Covid-19, which has arisen suddenly, “like a mist from the earth, and shed desolation on nations.” Speculation about the origin of Covid-19 has been capacious, including atmospheric change and animalcules, and most world governments have implemented policies based on the assumption “that the prohibition of direct intercourse with districts in which they prevailed would protect the inhabitants of a country from invasion.”
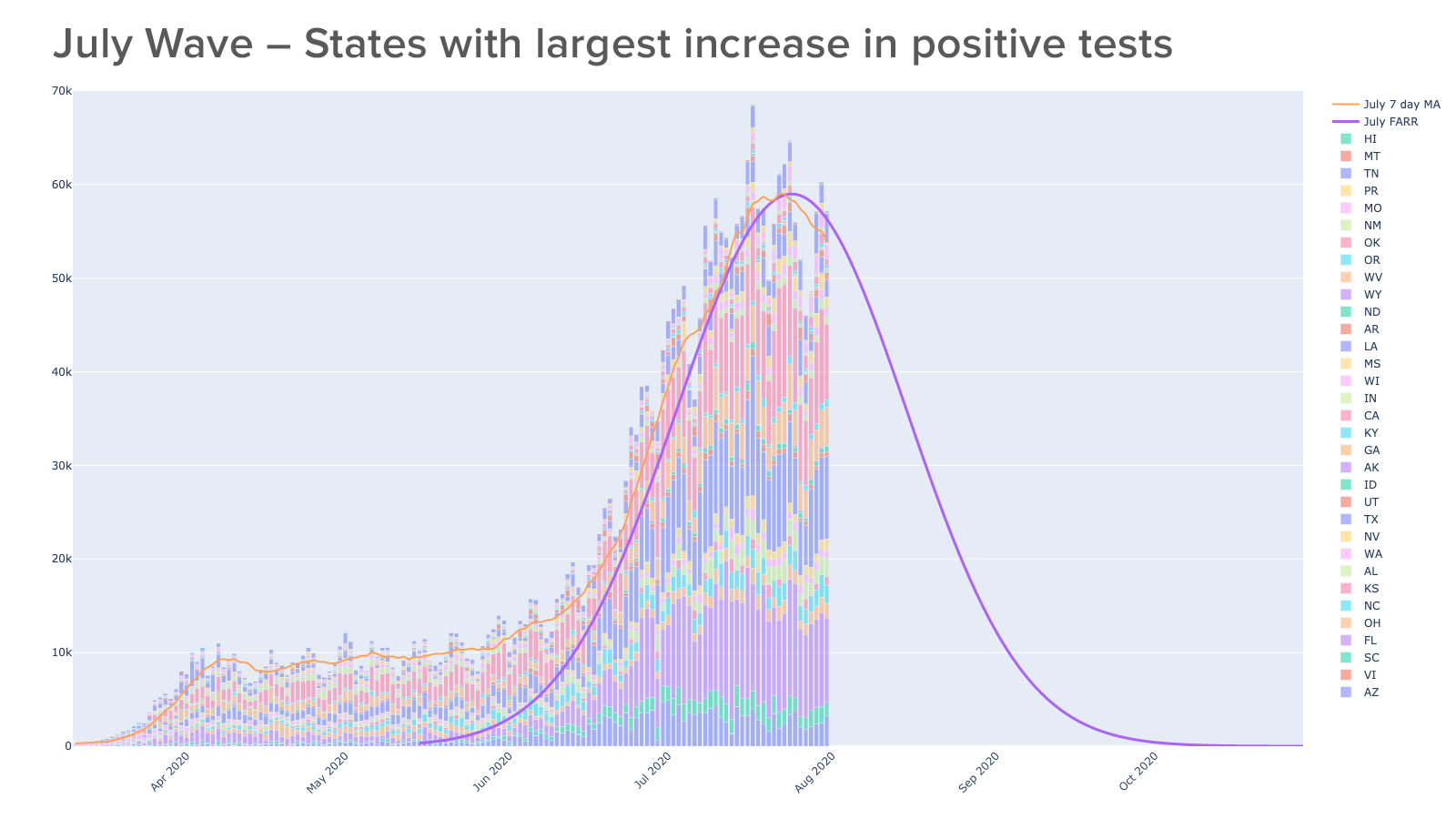
To apply Farr’s Law to the spread of Covid-19 in the United States, we grouped states (and territories) into “peak” months, using the day of each state's maximum increase in positive tests from data aggregated by The Covid Tracking Project (https://covidtracking.com). No state had a max day in June. We then fit a symmetrical curve to the plot, centering the peak on the cumulative max positive test day for the group. Based on this approach, states and territories fit into three distinct groups based on the peak of case positivity:
|
Peak Month |
Number of States and Territories |
List of States and Territories |
|
April |
12 |
Colorado, Connecticut, Delaware, Massachusetts, Michigan, New Jersey, New York, Pennsylvania, Rhode Island, Vermont, Guam, Northern Mariana Islands |
|
May |
10 |
District of Columbia, Illinois, Iowa, Maine, Maryland, Minnesota, Nebraska, New Hampshire, South Dakota, Virginia |
|
June |
0 |
None |
|
July |
34 |
Alabama, Alaska, Arizona, Arkansas, California, Florida, Georgia, Hawaii, Idaho, Indiana, Kansas, Kentucky, Louisiana, Mississippi, Missouri, Montana, Nevada, New Mexico, North Carolina, North Dakota, Ohio, Oklahoma, Oregon, South Carolina, Tennessee, Texas, Utah, Washington, West Virginia, Wisconsin, Wyoming, Puerto Rico, U.S. Virgin Islands |
The following graphs depict the application of Farr’s Law as noted above, with the first three graphs depicting the states and territories by their “peak” month, and the last graph showing the combined group.
Although we were not the first to suggest that Farr’s Law would apply to Covid-19, we were the first to suggest that the manner in which Covid-19 ravaged the New York metropolitan area was not a harbinger of what the rest of the U.S. would experience. The application of Farr’s Law seems to confirm our thesis; New York’s overall experience follows Farr’s Law but is exacerbated by a number of factors specific to the New York metropolitan area and compounded by the unknown unknowns of treating a novel virus.
Perhaps more importantly, the application of Farr’s Law to the experience in the United States over the past four months suggests that the widely held belief that the United States is in the midst of a “surge” or “resurgence” of Covid-19 is incorrect. As shown in the graphs above, there have been three distinct “outbreaks” of Covid-19 in the United States: one primarily centered in the Northeastern U.S., Colorado and Michigan; another that unfolded in the Upper Midwest and part of the Eastern Seaboard; and the current “outbreak” that is broadly dispersed throughout the rest of the United States, particularly the Sunbelt.
Finally, based upon the experience of the United States through July 31, it appears that the first two “outbreaks” have already tapered off in accordance with Farr’s Law, with the low, but persistent, case positivity in those two regions offering support for the notion that the pandemic is now endemic. [7] If Farr’s Law applies to the current “Sunbelt outbreak”, then it is likely to taper off in early October.
Whether in the future there will be a second wave of Covid-19, a true resurgence throughout the entire United States akin to the Spanish Flu, is beyond our purview. As William Farr said, “the death rate is a fact; anything beyond this is an inference.” We can only hope that Farr’s Law is correct, and that the positive case rate and infection fatality rate will continue to decline.
The general history of viruses also suggests that the virulence of Covid-19 will eventually abate in large measure. When that happens, hospitals will be the only institution in the world whose "new normal" is the "old normal."
One day, doctors and nurses will return to the "old normal" of knowing that they have chosen a profession that daily exposes them to innumerable harmful pathogens. They will be reminded that it is not the cause of death, but rather the loss of a life, that stirs their emotions. They will continue to serve others with the sobering knowledge that they have no idea of the symptoms or underlying illness of the next person who walks into the Emergency Department needing clinical care.
One day, and maybe and hopefully soon, physicians and nurses will not assume that the symptoms of the patient in front of them are caused by Covid-19, because the odds will be that something other than Covid-19 prompted that patient to seek care. And, eventually, the Chief Medical Officer will once again need to remind the medical staff that hand-washing hygiene is important.
According to a principle that has stood the test of almost 200 years, that day could be as soon as October. Is your system prepared to return to normal?
[1] Annual report of the Registrar-General of births, deaths, and marriages in England, 1838-1839, page 91
[2] https://www.cebm.net/covid-19/covid-19-william-farrs-way-out-of-the-pandemic/
[5] https://www.oxfordreference.com/view/10.1093/oi/authority.20110803095811145
[6] https://en.wikipedia.org/wiki/Bell_shaped_function
[7] https://www.sciencedirect.com/science/article/pii/S2666535220300306
{kind=link}
{kind=link}