






















.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)


Earlier this month, the Medicare Payment Advisory Commission (MedPAC) issued its June 2022 Report to Congress.1 MedPAC reiterates its recommendation that Medicare should base ambulatory payment rates on the safest and most efficient setting for a particular service (i.e., lowest-paid setting), rather than the current system, which incentivizes care delivery in the highest-paid setting.
Background
Since 2014, MedPAC has recommended several variations of this policy across 23 reports, which hospital and health system associations have vigorously opposed.2 ‘Site-neutral’ payment would give patients more flexibility in selecting sites of care, while reimbursement across settings would remain relatively consistent. Unequal ambulatory payment rates lead to increased spending without a differential impact on patient outcomes. 3 Of particular interest to MedPAC is the increase in spending that results from the acquisition of ambulatory providers by a hospital, even though the setting, staffing, and quality of the care delivered to patients does not change.
Analytic Approach
To evaluate the potential benefits of aligning payment rates across hospital outpatient departments, ambulatory surgical centers, and freestanding physician offices, MedPAC analyzed ambulatory payment classifications (APCs) used in the outpatient prospective payment system (OPPS). Using this data, the Commission determined which APCs could reasonably be set at physician fee service (PFS) rate levels (i.e., lowest-paid setting).
Findings
MedPAC identified 57 APCs for which “it would be reasonable to more closely align OPPS and ASC payment rates to PFS payment rates” because they generally require fewer resources and have been deemed safe to render across ambulatory settings. Alternately, 101 APCs were determined not to qualify for site-neutral payment because of a lack of appropriateness and safety, and thus would remain at higher payment amounts.
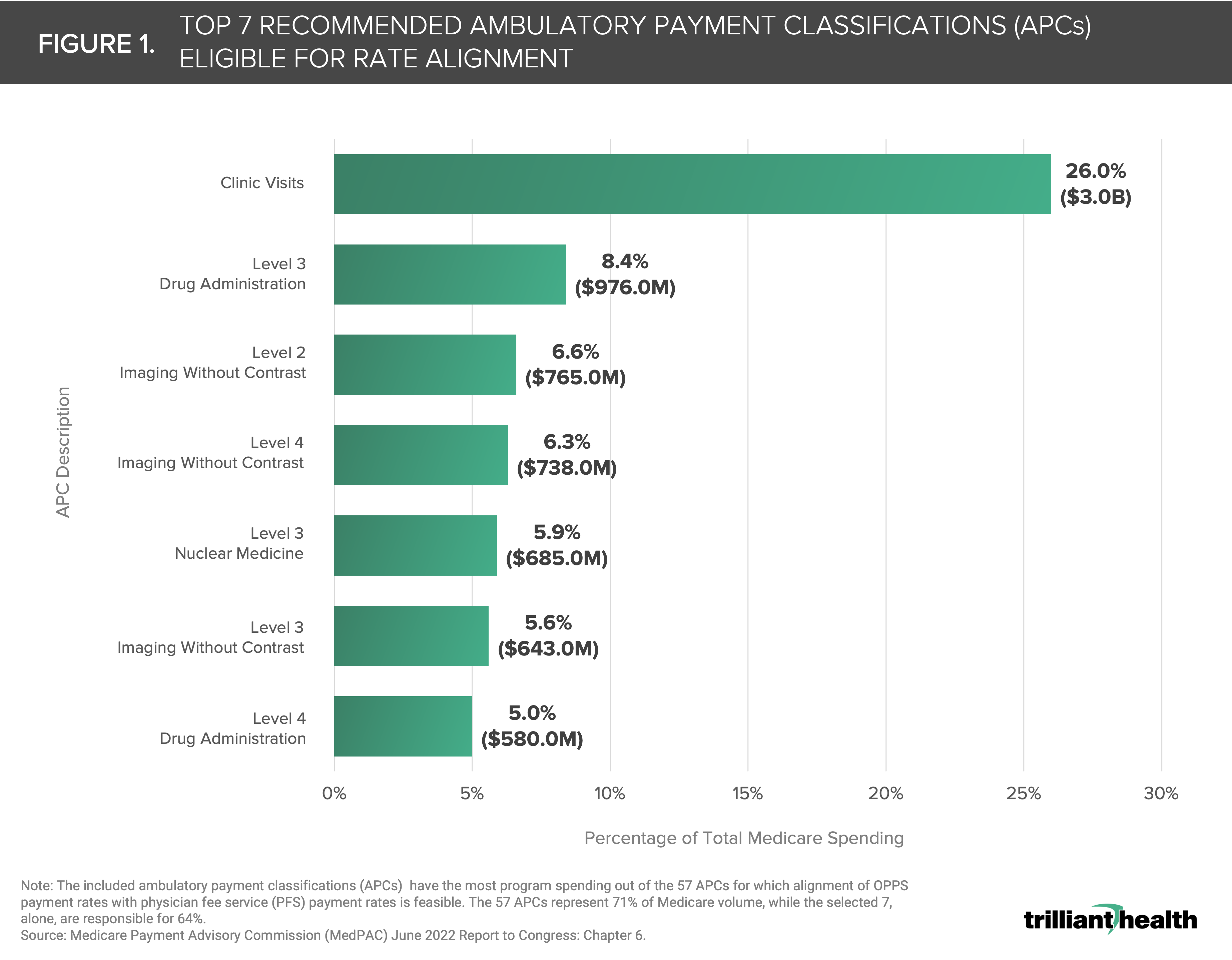
These 57 APCs represent 71% of total Medicare volume, the top seven of which are highlighted in Figure 1. Notably, the average OPPS payment rate for these 57 APCs is $149, which is far lower than the average OPPS APC payment rate ($381). Despite the lower than average per-visit payment rate, these 57 APCs account for more than $11.4B in annual Medicare spending. Among this group, clinic visits account for the largest single APC spending category, amounting to $3.0B annually (26%) (Figure 1). Spending, of course, does not equally correlate to visit volume. For example, level 3 drug administration has the second highest program spending but is in fourth in terms of visit volume. While not all services would be deemed clinically appropriate for site-neutral payment, the low-payment, high-volume services account for the bulk of MedPAC’s recommendation. Some research predicts that the adoption of site-neutral payments could decrease healthcare expenditures between $346B and $672B over the next decade.4
While the implementation timeline for site-neutral payments is unknown, it may still be wise for hospitals to proactively identify the potential near- and long-term budget impact. Rather than waiting for the law to change, could it be advantageous to make proactive, near-term rate changes to become the "price setter" in the market in which you operate?
The American Hospital Association has opposed site-neutral ambulatory payments, suggesting that equivalent costs across settings may result in unfair payment biases and reduced access to care for low-income and underserved beneficiaries.5 Other healthcare stakeholders, such as the Healthcare Financial Management Association (HFMA), have discussed the complexities of implementing site-neutral payment, indicating how current payment structures do not align with the diversification of care delivery settings, beyond the traditional inpatient setting.6
To that end, the debate around site-neutral care illustrates how payment structures, both in Medicare and commercial arrangements, do not reflect current care delivery trends. Longer term shifts from inpatient to outpatient settings remain unsettled with regards to payment stabilization in Medicare,7 and the rigidity of reimbursement models creates barriers to adopting novel healthcare technological advancements.8 As policymakers consider the recommendations of MedPAC and other stakeholders, a key consideration is how to equip healthcare payment systems to adapt to the rapidly changing healthcare environment. With healthcare increasingly being delivered outside of traditional care settings because of technological advances and concerns about cost, when will policy catch up? Or will that all be left behind?
Thanks to Katie Patton and Megan Davis for their research support.


