The Compass
Sanjula Jain, Ph.D. | November 10, 2024You are currently viewing the public version of Studies. To unlock the full study and additional resources, upgrade your subscription to Compass+.
Supply limitations are a defining feature of the U.S. healthcare system, impacting everything from provider and appointment availability to the accessibility of prescription drugs, durable medical equipment and medical supplies. Competition is intensifying for a smaller number of physicians, evidenced by the widening gaps in primary care physicians (PCPs), medical specialists and surgeons. The U.S. has far fewer PCPs than peer countries, with 0.31 PCPs per 1,000 population, while Canada has 1.33 and Australia has 1.77 PCPs per 1,000 population.1 By 2036, the gap in PCP supply is projected to range from 20,200 to 40,400 physicians, while the gap in hospitalists could range from a shortage of 1,300 physicians to a surplus of 4,900 physicians.2
The inadequate supply of providers, which is correlated with inadequate yield, will undoubtedly contribute to the already-worsening health status of Americans (Trend 5).
Competition Is Intensifying for a Smaller Number of Physicians
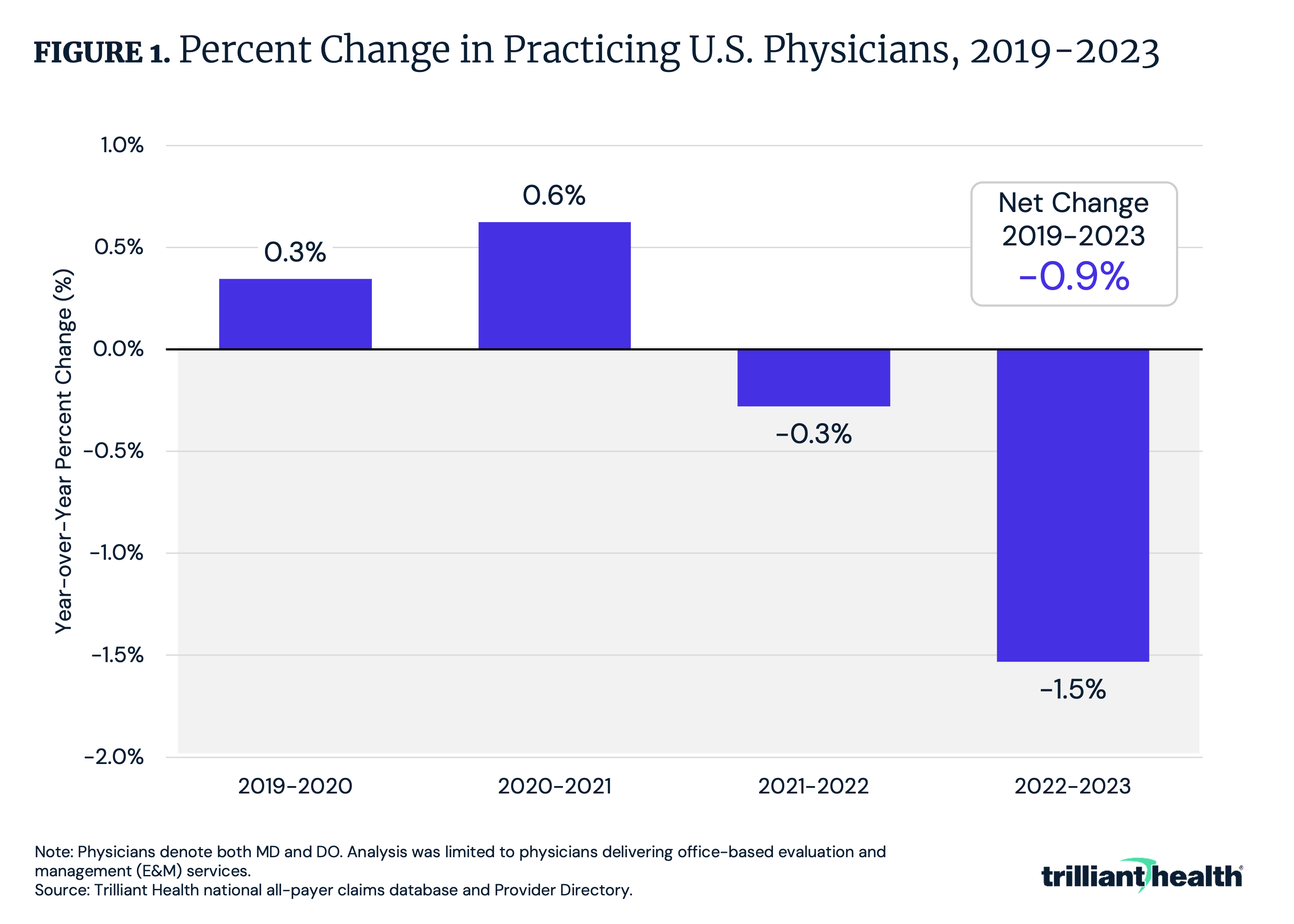
The current healthcare system does not incentivize adequate supply of providers but rather incentivizes supply where yield (i.e., profitability) is highest. This is further compounded by the fact that the net supply of physicians is declining. Leveraging our Provider Directory, we identified changes in national physician practice patterns and found that the net number of physicians that started and stopped practicing between 2019 and 2023 resulted in a -0.9% workforce reduction, with a workforce reduction of -1.5% from 2022 to 2023 (Figure 1). Additionally, 31.3% of physicians changed primary practice location between 2019 and 2023, whether a geographic relocation (i.e., from one health system to another), a change in practice type (i.e., traditional to retail provider) or “moonlighting” across organizations, particularly among virtual care providers. The increasing trend of physicians assuming non-clinical roles further intensifies competition, as it draws physicians away from the traditional clinical settings, putting strain on the already limited clinical workforce.
Even for Specialists that Are in “Adequate” Supply, Supply Is Not Evenly Distributed at the Market Level
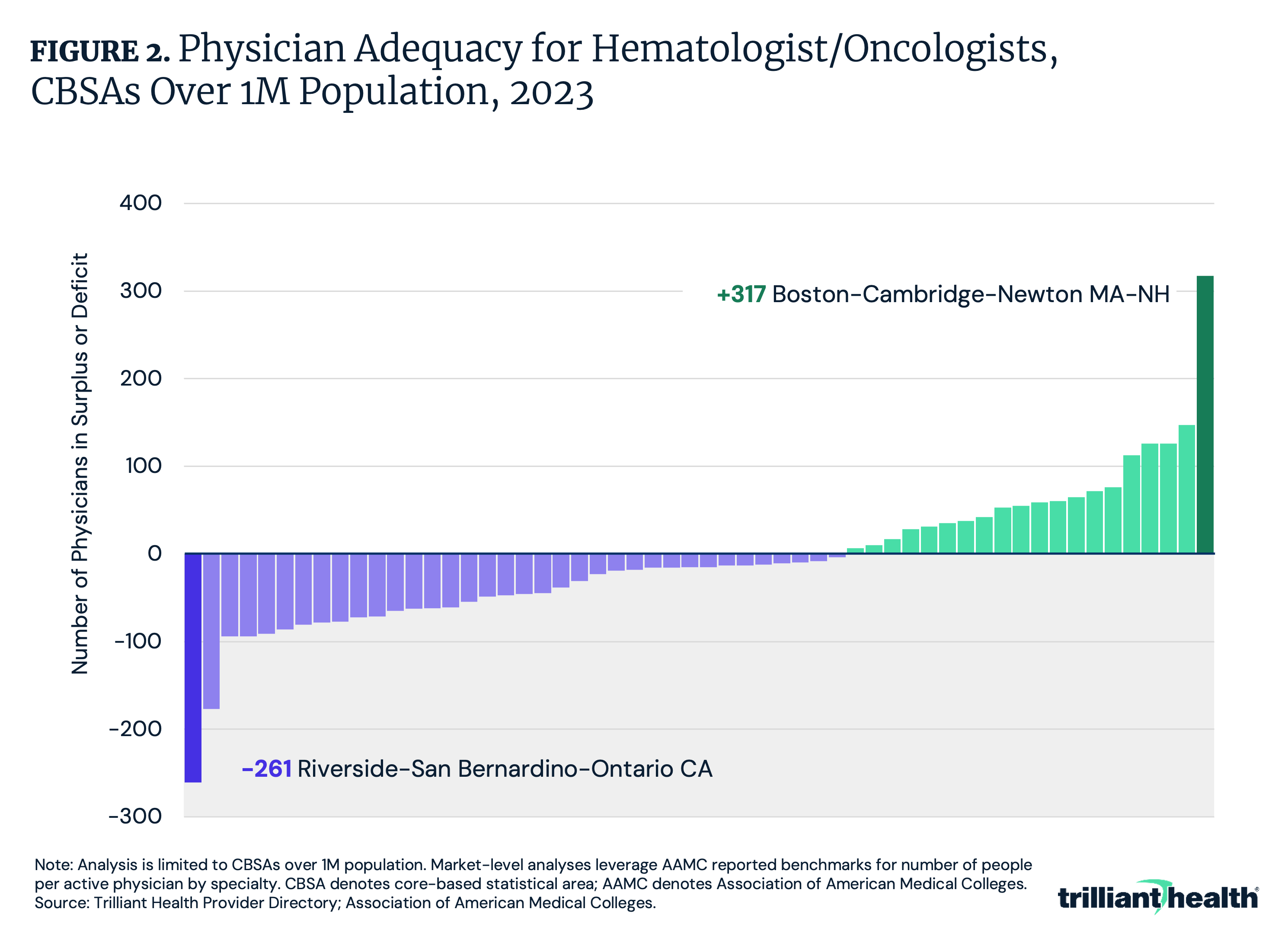
The current state of U.S. physician supply is characterized by factors such as burnout, an aging workforce, diversified employment opportunities and earlier retirements, resulting in a shortage of several provider types and physician specialties. We sought to explore the adequacy of physician supply at the market level for select specialties. In analyzing hematologist and oncologist supply in CBSAs with populations over 1M, 20 CBSAs have a population-based surplus of physicians, while 36 CBSAs have a population-based shortage, based on national-level Association of American Medical Colleges (AAMC) benchmarks (Figure 2). For instance, Boston has the highest surplus (+317 physicians), while Riverside has the largest shortage (-261 physicians).
The Majority of Physicians Are Employed, Not Independent
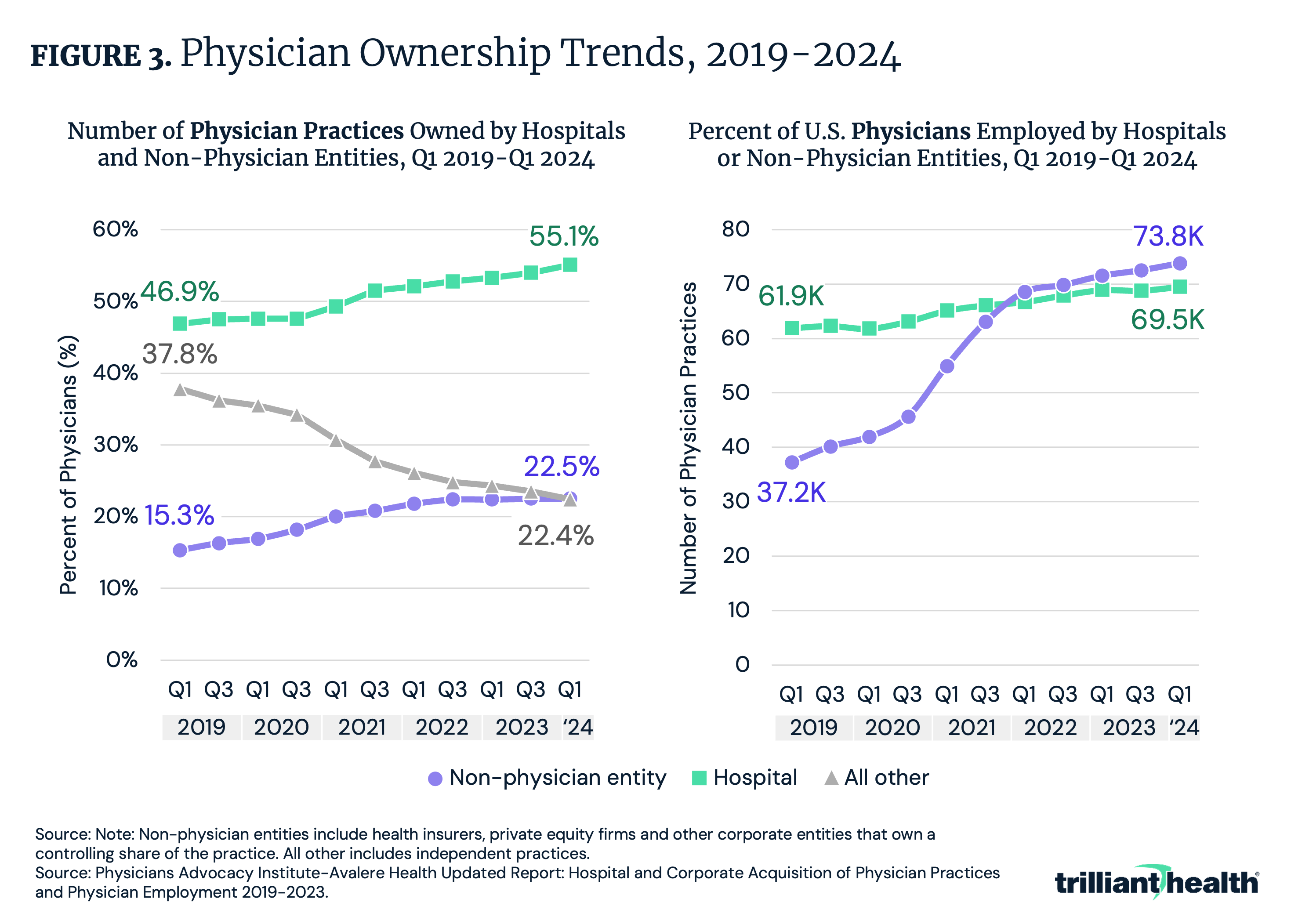
The intensifying competition for a declining number of physicians is further exacerbated by the growing employment of physicians by non-physician corporate entities, rather than hospitals or independent practices. Of physicians employed by a corporation, a growing share are employed by a non-physician entity (e.g., health insurer, private equity) rather than a hospital, increasing from 15.4% of physicians in Q1 2019 to 22.5% in Q1 2024 (Figure 3). This trend reflects a broader shift in practice ownership as well, given that, as of Q1 2024, more physician practices were owned by non-physician entities (73.8K practices) than by hospitals (69.5K practices). The rising influence of corporate ownership is reshaping the physician employment landscape and introducing new dynamics in care delivery and provider competition.
Upgrade to Compass+ to continue reading the full study.
- Primary Care
- Specialty Care
- Featured
- Healthcare Investments & Partnerships
- Healthcare Workforce
See more with Compass+
You are currently viewing the free version of this study. To access the full study, subscribe to Compass+ Professional for $199 per year.
Sign Up for Compass+Interested in citing our research? Please follow this guide.
