The Compass
Sanjula Jain, Ph.D. | October 27, 2024You are currently viewing the public version of Studies. To unlock the full study and additional resources, upgrade your subscription to Compass+.
Government innovation and regulation are often positioned as essential mechanisms for enhancing the value and efficiency of the healthcare system. However, it has become increasingly clear that these initiatives have not consistently achieved their intended outcomes. Building on the overarching thesis of the 2024 Trends Shaping the Health Economy Report that the U.S. healthcare system is disproportionately expensive and provides relatively little value, it is critical to examine the role of regulation.
This week, we examine the extent to which government-driven efforts to innovate and regulate the health economy have not sufficiently delivered value, defined as improved health outcomes relative to cost (Trend 3).
Effective Public Health Regulation Has Focused on Mortality Reduction
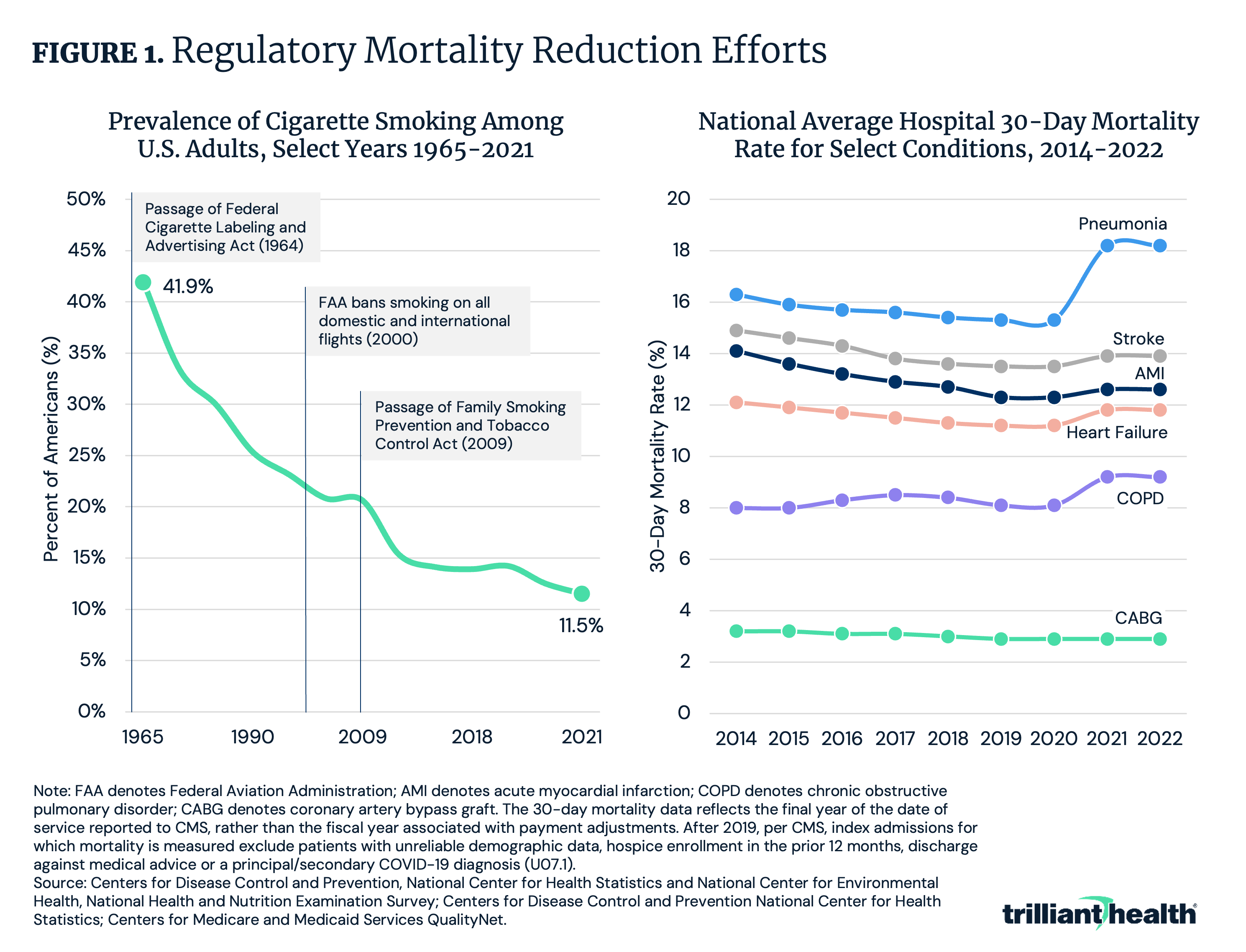
Relative to other areas of regulation, public health regulation has been more successful at achieving its aim: improving quality of life. For example, following the passage of legislation to regulate cigarette use – such as advertising restrictions, health warnings, increased taxation and public smoking bans – the prevalence of smoking decreased by 30.4 percentage points.
On the other hand, regulatory mandates requiring the reporting of healthcare quality measures have not produced commensurate outcomes (i.e., reductions in mortality or adverse healthcare events) at scale. While, on average, the hospital 30-day mortality rate declined from 2014 to 2022 by 1.5 percentage points for acute myocardial infarction and 1.0 percentage point for stroke, it increased by 1.9 percentage points for pneumonia and 1.2 percentage points for chronic obstructive pulmonary disease (Figure 1). The mandated reporting has contributed to increased administrative costs, but substantial improvements in mortality relative to these expenditures have not been observed. Consequently, the focus on mandated quality reporting may divert resources away from patient care without yielding proportionate benefits to health outcomes.
Quality Measurement Burden Remains High and Quality Reporting Requires Substantial Investment
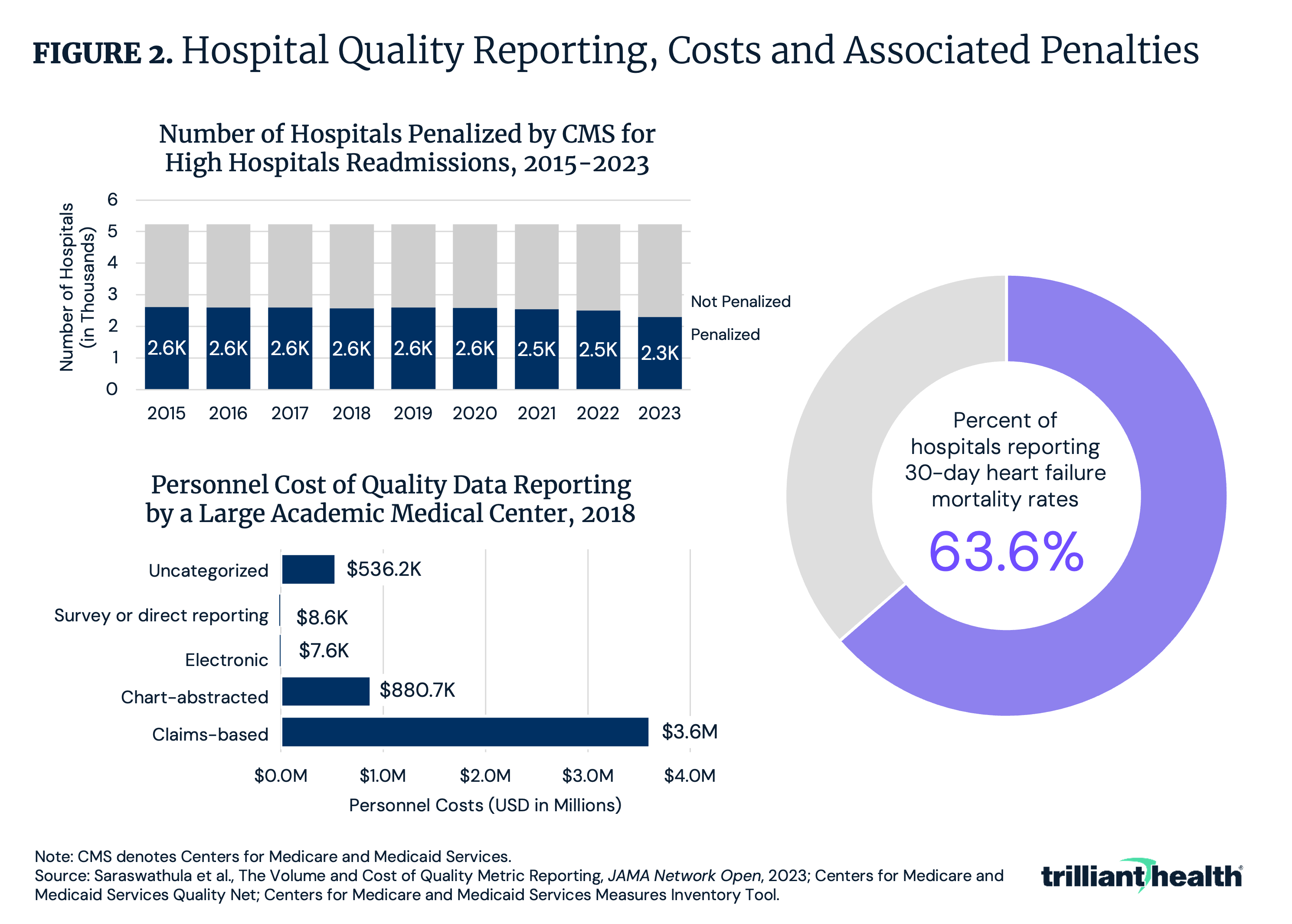
Many efforts to enhance care value, like quality reporting, are not systematically improving quality but are increasing spending. The Centers for Medicare & Medicaid Services (CMS) requires hospitals to report data on various quality metrics. However, the financial burden associated with these reporting requirements is substantial. A single academic medical center spent over $5.5M annually to track 162 quality measures (Figure 2). This high cost might explain in part why roughly one-third of hospitals did not report 30-day heart failure mortality rates, despite being required to do so. Relatedly, the share of hospitals penalized for not meeting readmission quality standards has remained around 50% since the inception of the CMS Hospital Readmissions Reduction Program in 2012. If CMS does not penalize those who fail to report and there is no observable improvement from those who do, then the effectiveness, if not underlying rationale, of these policies is questionable.
Value-Based Care Experimentation Has Persisted for More Than a Decade With Limited Uptake
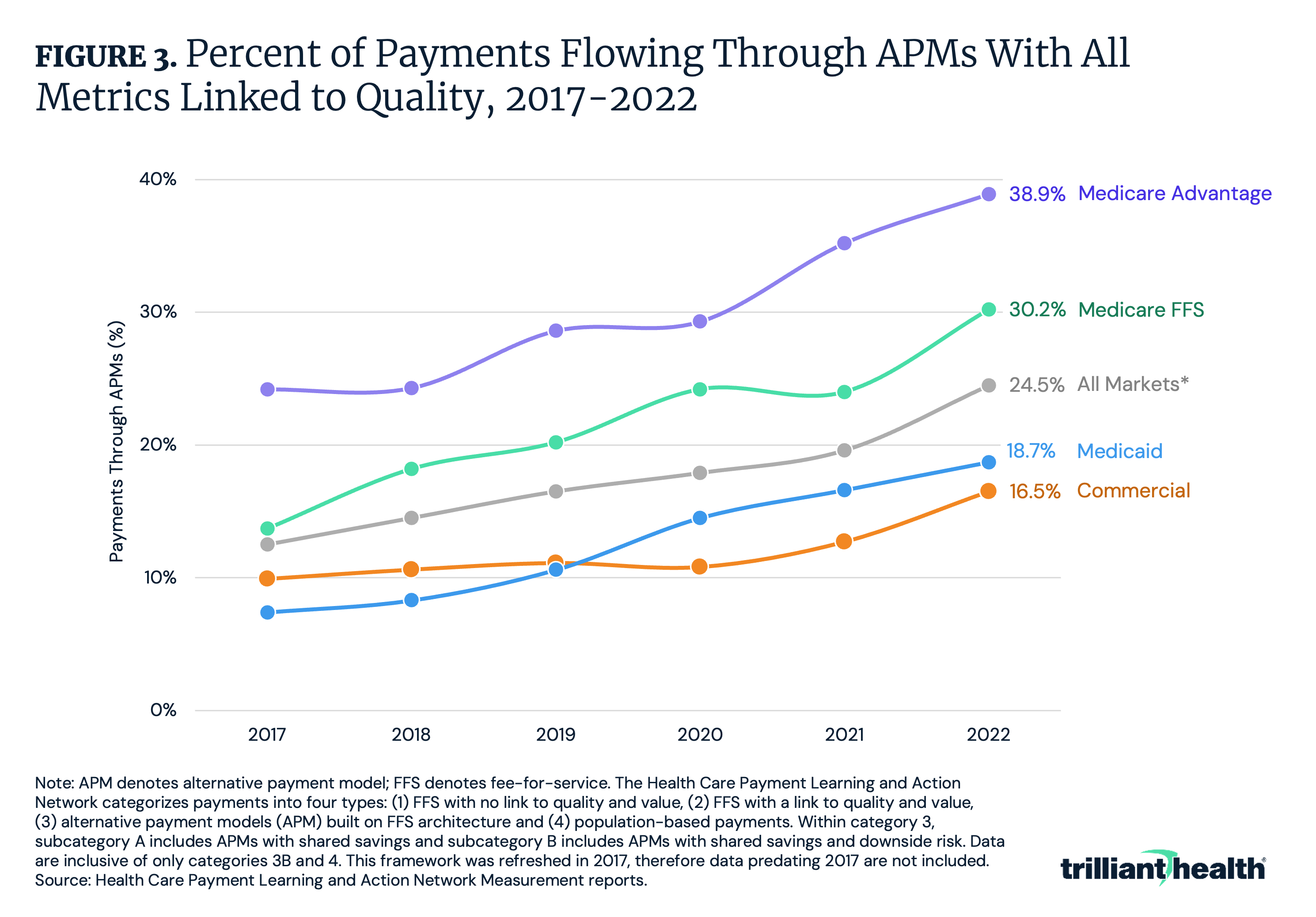
Despite years of value-based care (VBC) experimentation, its long-term viability as a strategy to reduce costs while improving quality remains in question. This is especially true given the structural and operational alignment between the U.S. healthcare system and fee-for-service (FFS) reimbursement. As of 2022, only 25.4% of U.S. healthcare payments flowed through value-based payment models, with Medicare Advantage representing the largest share (38.9%) (Figure 3). Moreover, VBC has taken hold the least in the commercial insurance market at 16.5%. Additionally, the savings generated by alternative payment models (APMs) administered by the CMS Innovation Center (CMMI), are not projected to offset expenditures, with $9.6B in net expenditures.1
A Substantial Share of Brand Drugs Receive Patent Extensions
Recent regulatory and administrative initiatives have been implemented to increase competition in the pharmaceutical industry to reduce drug prices.2,3,4 The Constitution grants Congress the power to protect intellectual property “for limited times,” but current patent law allows for extensions and other exclusivity mechanisms that delay the entry of lower-cost generics and biosimilars into the market, thus maintaining high drug prices for extended periods, which has significant implications for healthcare costs.5
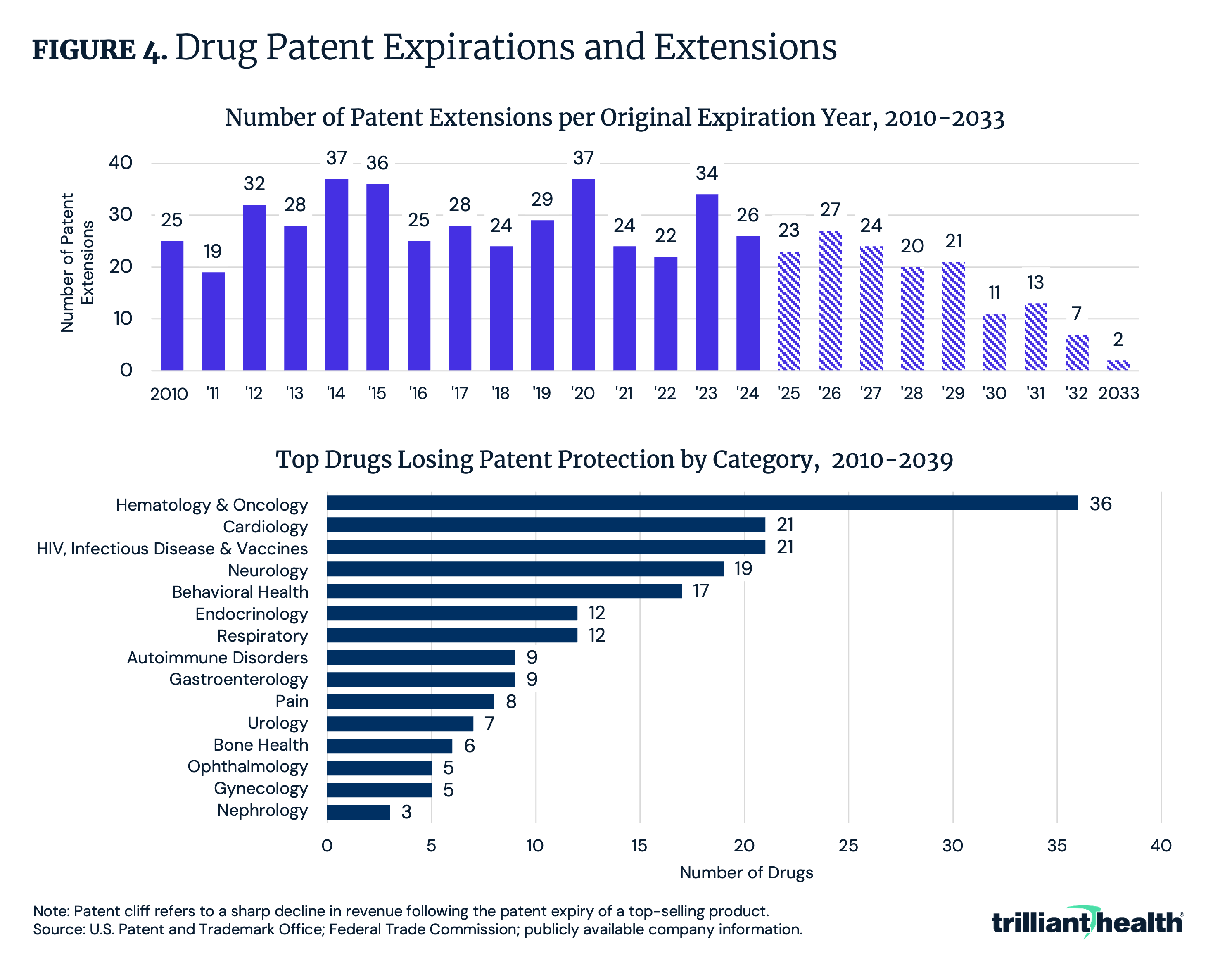
Between 2010 and 2033, 574 brand-name drugs have either received or are projected to receive patent extensions (Figure 4). Hematology and oncology drugs represent the largest share of medications expected to lose patent protection between 2010 and 2039, totaling 36 brand-name drugs. This category is followed by treatments for infectious disease, HIV, vaccines and cardiology. As these patents expire, manufacturers of high-revenue drugs – some generating up to $20B annually – are poised to face a substantial “patent cliff” over the next decade.
Upgrade to Compass+ to continue reading the full study.
- Health Reform
- Cost of Care
- Life Sciences
- Featured
- Quality & Value
- Disease Burden
See more with Compass+
You are currently viewing the free version of this study. To access the full study, subscribe to Compass+ Professional for $199 per year.
Sign Up for Compass+Interested in citing our research? Please follow this guide.
